Floods disrupt essential services and infrastructure including food, utilities and dwellings. These disruptions affect health outcomes and access to essential health services. The increasing incidence of severe weather events has been linked to climate change (IPCC 2022) and highlights the importance of a climate-resilient health system to provide timely services. This paper considers the immediate effects that a severe flooding event within Nepean Blue Mountains Local Health District (NBMLHD) had on emergency health utilisation to inform future health planning and facilitate the evaluation of climate responsive interventions.
Introduction
The Hawkesbury-Nepean Valley of New South Wales has a complex and high flood exposure risk; one of the highest in the state. It is considered particularly vulnerable at choke points along the river that results in upstream flooding (Herron et al. 2018). In March 2021, heavy rainfall caused significant water outflow from the Warragamba Dam that resulted in a 1 in 10 to 20 chance per year flood downstream at the urban centres of North Richmond, Windsor and Sackville (Infrastructure NSW 2021). The flood damage caused riverbank erosion, road and bridge closures, it isolated communities north of the river and limited access to essential infrastructure (Infrastructure NSW 2021). It was reported that 65,000 people across Sydney were affected by evacuation warnings and orders during this time (National Recovery and Resilience Agency n.d.). An estimated 1,230 dwellings, commercial buildings and homes in caravan parks were inundated in the Hawkesbury and Penrith regions (Infrastructure NSW 2021).
The direct health effects following a flood event include drowning, injury, hypothermia, carbon monoxide poisoning and infectious diseases, specifically gastroenteritis secondary to contaminated drinking water, skin infections and vector- or rodent-borne diseases (Paterson et al. 2018; Ahern et al. 2005, Saulnier et al. 2017). Other indirect health effects can arise due to treatment interruption due to limited access to services or medications and poor nutrition (Paterson et al. 2018; Saulnier et al. 2017). Mental health conditions can also occur but are more likely in the longer term (Mulchandani et al. 2020).
There is limited evidence available that assesses the effects of floods on health outcomes and, due to the challenges in researching high-risk hazards and disasters, research often relies on observational data (Public Health England 2014). Globally, emergency department (ED) presentation data has been used in various flood and storm events to evaluate health outcomes. Following Hurricane Sandy in New York, Lee et al. (2016) demonstrated transient reductions followed by overall increases in presentations to EDs in the 4 days following the event with subsequent analysis by Doran et al. (2016) showing that there was a disproportionately higher number of presentations related to social factors such as homelessness and inadequate housing in the weeks following the event. ED presentations for dermatitis (Chen et al. 2021), skin infections (Saulnier et al. 2018), gastroenteritis (Wade et al. 2014, Saulnier et al. 2018), injuries (Sahni et al. 2016) and drowning (Ogden et al. 2001) have also been reported to increase after flood events. While acute cardiovascular and respiratory conditions have been shown to increase during storms, available evidence is limited in the context of floods (Saulnier et al. 2018).
An observational study was undertaken to understand health service utilisation for flood-related health issues and, therefore, inform future health planning in a notoriously flood-prone area.
Methods
A retrospective, observational, before-after study was conducted of people who presented to EDs from flood-affected postcodes in NBMLHD between 24 January and 22 May for the years 2015, 2017, 2018, 2019 and 2021 and between 25 January and 22 May for 2016 (due to the leap year).
Data was accessed via the Secure Analytics for Population Health Research and Intelligence platform (NSW Health 2022a) and was extracted from the Emergency Department Records for Epidemiology dataset. This dataset is a compilation of data from almost all EDs in New South Wales (several small rural hospitals and multi-purpose facilities are not covered) (NSW Health 2022b). SAS Enterprise Guide 9 was used to access de-identified data. Further analysis of aggregated data was done with Microsoft Excel and confidence intervals were calculated with a web-based rate ratio calculator, OpenEpi (Sullivan & Dean 2008).
Flood-affected postcodes (2745, 2750, 2753, 2754, 2755, 2756, 2758, 2765 and 2775) were defined as the suburbs within NBMLHD that had greater than 20 inundated dwellings, greater than 10 dwellings isolated by flooding or had flood levels reaching a major flood definition (Infrastructure NSW 2021). The flood dates were characterised by the period of major flooding from measured water levels (Infrastructure NSW 2021). The study periods were subsequently defined as:
- pre-flood reference period (24 January–20 March)
- flood period (21 March–27 March)
- first month post-flood (28 March–24 April)
- second month post-flood (25 April–22 May).
Daily presentation incidence ratios were calculated for flood and post-flood periods relative to the pre-flood reference period for 2021. The same calendar dates were analysed as comparative periods for non-flood years (2015–19). Even though there was no flooding in these years, the same nomenclature was retained for these comparative calendar periods. ED presentations in 2020 were excluded due to that year’s minor-to-moderate flooding as well as significant bushfires occurring in the region. There was sub-group analysis by demographic (age and gender), triage groups and diagnostic classification groups of interest defined by ICD-10/SNOMED codes (Public Health England 2014). All SNOMED codes were mapped to ICD-10 (SNOMED International 2022) to facilitate comparison and amalgamation of data.
Ethics approval for this study was obtained from the NBMLHD HREC (2022/ETH01439).
Results
The total population residing in the affected postcodes within NBMLHD local government areas in 2021 was estimated as 163,837 people (51% female and 49% male; 10% were under 5 years of age and 15% were 65 years and over). Population mix was calculated based on Australian Bureau of Statistics 2021 Census data (Australian Bureau of Statistics 2021). The proportion of presentations to EDs by age and gender for pre-flood to post-flood periods were calculated and noted to be similar across the calendar periods (Table 1).
Table 1: Population characteristics during the study periods in flood and pre-flood years.
| Age | 2021 | 2015-19 |
| Under 5 years | 10% | 11% |
| 5 – 64 years | 67% | 67% |
| 65 years and over | 22% | 22% |
| Gender | ||
| Male | 50% | 51% |
| Female | 50% | 49% |
The total daily ED presentations were higher in the second month post-flood (rate ratio 1.04 [95%CI 1.02–1.07]) whereas they declined in the comparative non-flood period (rate ratio 0.88 [95% CI 0.87–0.88]) (Table 2). There was a reduction in the daily presentation rates during the flood (rate ratio 0.87 [95% CI 0.83–0.91]) and first post-flood month (rate ratio 0.97 [95% CI 0.95–0.99]), consistent with the comparative non-flood years (rate ratio 0.97 [95% CI 0.96–0.98]). However, the rate ratio reduction for the flood year was more marked.
The rate ratio for high-urgency presentations (triage categories 1, 2, 3) were higher in the second post-flood month (rate ratio 1.06 [95% CI 1.03–1.10]). During the flood period, the reduction in high- urgency presentations (rate ratio 0.86 [95% CI 0.81–0.92]) was more marked compared to non-flood years (rate ratio 1.00 [95% CI 0.98–1.02]). In the non-flood years, low-urgency presentations (triage categories 4, 5) reduced during the second month post-flood dates. However, there was no difference for the flood year during the same period (rate ratio 1.02 [95% CI 0.99–1.06]), which suggests a relative increase in lower category presentations.
There were no significant changes in the presentation rates for NBMLHD hospitals during the flood and post-flood periods (Table 2). However, there were increased presentations to out-of-area hospitals during the flood (1.15 [95% CI 1.02–1.21]) and during the first post-flood month (1.08 [95%CI 1.01–1.17]) and second post-flood month (1.09 [95%CI 1.01–1.17]).
Table 2: Rate ratios for total ED presentations per day by triage category and hospital location for flood year 2021 and non-flood years 2015–19*.

* Rate ratios for all periods are calculated relative to the pre-flood reference period. Statistically significant increased ratio of presentations (orange), statistically significant decreased ratio of presentations (blue). Pre-flood period: 24 Jan to 20 Mar (25 Jan to 20 Mar for 2016).
Flood period: 21 Mar to 27 Mar. First post-flood period: 28 Mar to 24 Apr. Second post-flood period: 25 Apr to 22 May.
The diagnostic classification groups of ED presentations showed some difference in the flood and post-flood periods when compared to non-flood years (Table 3). Respiratory and cardiovascular presentation rates increased but no significant trends were seen with gastroenteritis, dermatological conditions, injury and trauma, chemical and poisoning or mental health when compared with the preceding non-flood year trends.
An increase in respiratory presentations in the first (rate ratio 1.42 [95%CI 1.27–1.59]) and second months (rate ratio 1.72 [95%CI 1.55–1.92]) following the flood was noted. In comparison, an increase in respiratory presentations during the corresponding periods in the non-flood years was noted. However, during the flood year the increase in presentations was more marked with the greatest rate ratio increase seen in the second post-flood month (Table 3).
Table 3: Rate ratios for ED presentations per day by diagnostic classification groups for flood year 2021 and non-flood years 2015–19*.
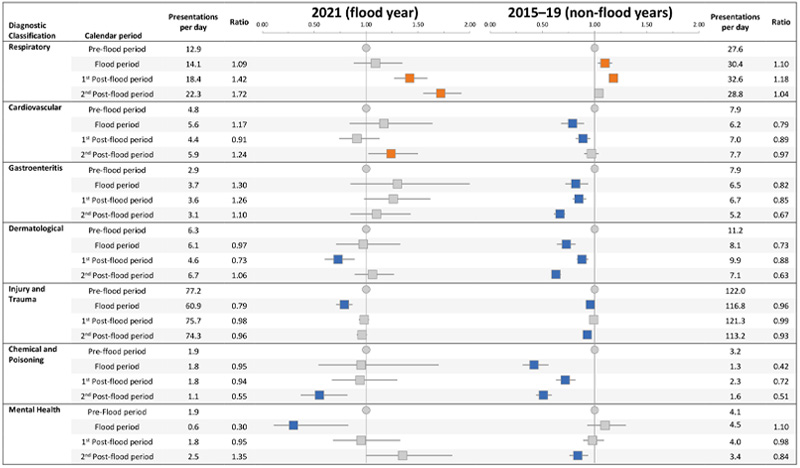
* Rate ratios for all periods are calculated relative to the pre-flood reference period. Statistically significant increased ratio of presentations (orange), statistically significant decreased ratio of presentations (blue). Pre-flood period: 24 Jan to 20 Mar (25 Jan to 20 Mar for 2016).
Flood period: 21 Mar to 27 Mar. First post-flood period: 28 Mar to 24 Apr. second post-flood period: 25 Apr to 22 May.
Cardiovascular presentations were higher in the second post-flood month (rate ratio 1.24 [95% CI 1.02–1.50]). In comparison with non-flood years there was no difference seen in the same calendar dates.
There was a reduction in injury and trauma presentations during the flood period (rate ratio 0.79 [95%CI 0.71–0.87]), which was more marked when compared to the corresponding non-flood years (rate ratio 0.96 [95% CI 0.93–0.99]). The reduction in chemical and poisoning presentations in the second month post-flood was comparable with the non-flood years.
Discussion
When compared to non-flood years, the increase in total ED presentations in the post-flood period suggests that the flood may have affected ED presentations patterns in the district. The reduction of ED presentations at the time of the flood is consistent with the findings from Lee et al. (2016) that showed there is a transient reduction in presentations at the time of the event followed by an increase in ED utilisation in the most-disaster prone regions. However, in this study, the increases were seen 2 months after the event in contrast to a few days, as reported by Lee et al. (2016). This may be explained by the longer duration of the study periods such that a granular variation may not have been identified in the analysis.
In addition to identifying reduced ED presentations during the flood, this study captured the number of people who presented to out-of-area hospitals where there was a significant increase in ED presentations, indicating that there may have been barriers to accessing hospital services. Standing evacuation orders and messages regarding avoiding the area (Pearce and Marsh 2021) may have diverted residents away from NBMLHD hospitals and the isolation of the North Richmond area (Infrastructure NSW 2021) may have re-directed residents to out-of-area hospitals. Further, a temporary medical service was deployed to the isolated North Richmond area to triage critical patients and provide medical support while patients awaited transfer to tertiary care (NBMLHD 2021). The service was not open to walk-in patients and non-critical patients were redirected to their general practitioner or community pharmacies (NBMLHD 2021).
Flood awareness campaigns and messaging promoting preparedness and resilience during 2019 and 2020 (Infrastructure NSW 2021) may have also potentially reduced community reliance on EDs. The introduction of telehealth in primary care in Australia since the COVID-19 pandemic (Australian Department of Health and Aged Care 2022) may have introduced greater capacity in the primary care system, relieving the pressure on tertiary services, such that treatment for minor illnesses or prescriptions were accessible by phone.
While this study identified the effect on some acute presentations, the duration of follow-up may not have been sufficient to identify conditions with longer latency, such as mental health. The results showed mental health presentations reduced during the flood year (Table 3) and there was no difference in the post-flood period. However, Mulchandani et al. (2020) demonstrated that the effects of floods on mental health can take years to be identified. It is uncertain what the consequences will be of repeated flooding events on the baseline mental health incidence for the residents living in flood-prone areas (Mental Health Commission of NSW 2022).
There were also consistent reductions in gastroenteritis presentations during the flood and post-flood periods for the non-flood years, but no difference was seen during the flood year (Table 3). This suggests that gastroenteritis may have increased after the flood relative to the comparative non-flood years. However, the interpretation of this finding is uncertain and as daily case rates were low (as was the case for mental health presentations) and there may have been insufficient statistical power to demonstrate a significant difference. In a systematic review by Saulnier et al. (2017), there were several studies showing onset dates of gastrointestinal illness up to 7 weeks after the flood with 10–54% of treatment facility presentations being related to gastroenteritis. However, this was based on studies located in low- and middle-income countries and may not be generalisable to the Australian context.
Cardiovascular presentations have been shown to increase after disaster events and are thought to be related to the direct physical and emotional stress and the indirect effects of treatment interruption (Babaie et al. 2021). This could explain the increase in cardiovascular presentations noted in the post-flood period in this study.
The marked increase in respiratory presentations, particularly in the second month post-flood period, may have been related to heavy rainfall and flooding causing increased mould exposure triggering allergic rhinitis and asthma as identified by Takaro and Henderson (2015). Despite this study being undertaken during the pandemic, COVID-19 case numbers were stable with only 9 locally acquired cases and no community transmission identified throughout the study period (NSW Health 2021b).
This study attempted to account for the influence of the pandemic in several ways. Firstly, rate ratios were calculated before and after the flood, when the case rates were stable in New South Wales and COVID-19 was likely to affect pre- and post-flood periods in the same way. Secondly, the study design ensured that the follow-up period did not overlap with the emergence of the Delta variant wave. Finally, 2020 was excluded from the analysis due to bushfires and flooding and also due to the effects of the pandemic restrictions on ED presentations in that year. While these effects returned to pre-COVID ranges by 2021, there were significant decreases in ED presentations in March 2020 at the start of the pandemic (Australian Institute of Health and Welfare 2021) and similar effects were seen for presentations for gastroenteritis and bronchiolitis, which likely decreased due to hand hygiene and social distancing measures (NSW Health 2021a).
The study of disaster events can be challenging when there is such heterogeneity in flooding events, especially when the timing and degree of flooding cannot be predicted. Exposures may vary in the extent of inundation, infrastructure damage, geographic location, promptness of warnings and may occur in conjunction with other weather events, amalgamating into an event that may be unique (Public Health England 2014). Therefore, use of routinely collected data allows for baseline and post-flood evidence and this methodology is better placed to retrospectively evaluate the demand on EDs after a flooding event. The use of routine ED presentation data can be considered reliable because activity-based funding requires administrative data to be collected (National Health Funding Body 2021).
There are limitations with ED presentation data. Emergency department presentation patterns vary seasonally and this study attempted to address this by comparing patterns to years that pre-dated the pandemic and the major flood event. Diagnostic classifications and residential postcodes are limited by potential coding or data collection errors, particularly for people who may have been displaced or evacuated (Public Health England 2014). ED presentation data is skewed towards high-severity disease and is likely to underrepresent low-severity illness and people may present elsewhere for treatment. The use of varied health data sources allows for the identification of different severity disease and, for future studies, such sources could include routinely collected data for mortality, clinical toxicology consultations, laboratory, syndromic surveillance, primary care, prescriptions and community survey data (Public Health England 2014).
The use of postcode boundaries is also unlikely to represent residents who are equally affected by the flood. As such, a study that analyses a cohort of people residing in non-flood affected areas may have allowed for direct comparison to better control for confounders such as the pandemic and weather conditions.
Conclusion
The propensity for flooding in the Hawkesbury-Nepean Valley combined with the increasing frequency of extreme weather events requires future service planning to be responsive to the effects of major flooding events on EDs. This study demonstrated an increase in ED presentations in the second month after the 2021 flood and relative decreases in ED presentations during the flood period. There was an increase in high-triage category presentations in the second month post-flood and a relative increase in out-of-area hospital presentations during and after the flood. Respiratory and cardiovascular presentations were shown to increase in the post-flood period with no meaningful findings for mental health, chemical and poisoning, injury and trauma, dermatological or gastroenteritis presentations. These results suggest that there are likely effects for tertiary healthcare service delivery during and after major flooding. This study highlights the importance of service delivery planning and messaging during the post-event recovery period. Research to understand the effects of floods on primary care and long-term chronic health conditions would be beneficial.