Earthquake preparedness in South Australia: recommendations based on previous earthquakes in Australia, New Zealand and the United States of America
Olga Anikeeva, Malinda Steenkamp, Paul Arbon
Peer-reviewed Article
Abstract
Adelaide is the most earthquake-prone capital city in Australia, with earthquakes of a magnitude five to six on the Richter scale occurring frequently enough to be a potential danger. This paper explores the short and long-term physical and psychological consequences of earthquakes that have occurred in settings comparable to metropolitan Adelaide in order to make recommendations in terms of the lessons learned. The danger posed by unreinforced masonry buildings in Adelaide is highlighted and the importance of effective communication and collaboration between local and national providers of essential services is discussed. The paper concludes with recommendations, including the development and rehearsal of emergency plans, community education and preparedness, planning for longer-term health outcomes and availability of practical and financial support.
Article
Introduction
Although Australia experiences few earthquakes by world standards (Gibson 2010, McCue 2010), Adelaide is the most earthquake-prone city on the continent, with moderate earthquakes (magnitude five to six on the Richter scale) occurring frequently enough to be a potential danger (Doyle et al. 1968). In the past 150 years, 15 earthquakes of magnitude five or greater were recorded in South Australia. Earthquakes of this magnitude lead to damage in the epicentre zone and can be felt over an area with a radius of approximately 200 km (Greenhalgh et al. 1994).
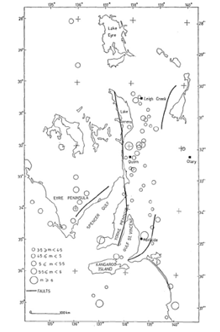
Earthquakes in South Australia primarily occur within two belts:
- the Adelaide seismic zone extending from Kangaroo Island, through the Mount Lofty and Flinders Ranges, to Leigh Creek in the state’s north, and
- the Eyre Peninsula zone (Doyle et al. 1968, Sutton & White 1968, Greenhalgh et al. 1994) (Figure 1).
Figure 1: Map of earthquake epicentres in South Australia (Doyle et al. 1968).
Earthquakes occurring in urban areas pose a risk to residents and essential societal systems, including critical infrastructure (World Association for Disaster and Emergency Medicine 2003, McCue 2010). If an earthquake of a similar magnitude to the 1954 Adelaide earthquake (5.4 on the Richter scale) were to occur today, it would result in substantial loss of life, injuries and damage, with losses over AUD$1 billion (Greenhalgh et al. 1994).
Aim
This paper examined earthquakes that have occurred in settings comparable to the physical and social environment of metropolitan Adelaide to make recommendations for South Australia in terms of lessons learned. The focus was on at-risk population groups and lifelines and the short and long-term consequences of selected events, including fatalities, injuries, psychological impact and damage to infrastructure.
Methods
A recent comprehensive review article by Doocy and colleagues (Doocy et al. 2013) was used for identifying relevant articles. Additional searches were performed on Medline, Scopus and Google Scholar to identify papers published after the period covered by the article. Earthquakes were selected based on the similarities of their location and environment to the South Australian context in terms of building stock, demographics and level of development. The details of the selected earthquakes are presented in Table 1. The South Australian Government State Emergency Management Plan (State Emergency Management Committee 2012) served as a starting point for the recommendations made in this paper.
Table 1: Summary of included earthquakes.
|
Location |
Event |
Magnitude (Richer scale) |
Day of week and time of day |
Fatalities and injuries |
Psychological impact |
Impact on infrastructure |
|
Australia |
Adelaide 1954 |
5.4 |
Monday 3:40 am |
0 fatalities 16 injuries |
Not reported |
30 000 insurance claims filed. Widespread structural damage. |
|
Newcastle 1989 |
5.6 |
Thursday |
13 fatalities 105 injuries |
20% of population sought formal support. Psychological morbidity still detectable after two years. |
78 full and 173 partial demolitions. 1 161 buildings deemed a danger to the public. 3 812 buildings damaged, but habitable. |
|
|
New Zealand |
Christchurch 2010 |
7.1 |
Saturday :35 am |
0 fatalities 2 injuries |
Depression, anxiety, stress and sleep deprivation more common among those affected by earthquake. |
Two buildings collapsed and many partially collapsed, with unreinforced masonry buildings performing very poorly. |
|
Christchurch 2011 |
6.3 |
Tuesday 2:51 pm |
185 fatalities 6,659 injuries |
Not reported |
Two multi-storey office buildings collapsed, many more buildings partially collapsed. |
|
|
California |
Loma Prieta 1989 |
7.1 |
Tuesday 5:04 pm |
63 fatalities 3 757 injuries |
Not reported |
Elevated freeway collapse, bridge damage, widespread structural damage. |
|
Northridge 1994 |
6.7 |
Monday 4:31 am |
57 fatalities 7 000 injuries |
Lower psychological symptoms among older residents. |
Substantial damage to power lines, roads, bridges and property. |

Image: Newcastle City Council
Demolition of Newcastle Workers Club, the scene of the greatest damage to any building in Newcastle where nine people died and many others were injured.
Discussion
Australia
Australia has experienced a number of destructive earthquakes in the past, most notably the 1954 Adelaide and 1989 Newcastle events that caused widespread damage to housing and commercial structures, particularly unreinforced masonry buildings (Doyle et al. 1968, Gibson 2010). The Adelaide earthquake led to over 30 000 insurance claims being filed and the Newcastle earthquake resulted in between $900 million and $1.5 billion of property damage (Lewin et al. 1997). While the 1954 Adelaide earthquake did not result in any deaths and caused only 16 injuries (McCue 2010), the Newcastle earthquake caused 13 fatalities (Greenhalgh et al. 1994). In total, 105 individuals received injuries that were treated in Newcastle’s public medical centres, with 30 of the injured being admitted to hospital. The main causes of injury included contusions and bone fractures. A further 800 people required emergency accommodation.
In the first month following the earthquake, 78 full and 173 partial demolitions were approved, 1 161 buildings were deemed a danger to the public and 3 812 were damaged but habitable. Several of the damaged structures housed important public infrastructure associated with essential services. The Royal Newcastle Hospital was evacuated due to structural damage, while two other hospitals and the City Fire Station and Ambulance Office sustained some damage, impacting on their ability to provide services (Carr et al. 1997).
The Newcastle earthquake was of moderate magnitude (5.6 on the Richter scale) and was the first recorded earthquake in Australia to result in loss of life. In the first six months following the earthquake, over 20 per cent of the adult population in Newcastle used general and/or disaster-related support services. Nearly 60 per cent used personal sources of support, including family, friends and neighbours, with over one-third of the population relying exclusively on these informal supports (Carr et al. 1997). However, the frequency of visits to doctors did not increase in the six month period, suggesting that earthquake-related issues were dealt with during consultations for other matters. Psychological problems were found to decline over time, but tended to stabilise at approximately 12 and 18 months for general psychological illness and trauma-related mental illness, respectively. Those who sustained injuries in the earthquake exhibited the highest level of distress. The degree of initial earthquake exposure (avoidance coping style, traumatic life events since the earthquake, ongoing disruptions, older age, a history of emotional problems and poor social relationships) contributed to ongoing psychological issues two years after the event (Carr et al. 1997).
New Zealand
While New Zealand differs from Australia in terms of earthquake frequency and severity (McCue 2010), there are similarities between the healthcare systems in each country considering building stock and demographics. Thus, the two recent earthquakes in Christchurch can inform planning in South Australia.
The first of the New Zealand events occurred 30 km west of Christchurch on 4 September 2010 at 4:35am, with frequent and unpredictable aftershocks continuing for months. The earthquake did not result in any fatalities, but caused two serious injuries. This was attributed to the performance of most modern buildings and the early morning occurrence, which meant that most residents were away from the business districts of Christchurch and Kaiapoi (Wood et al. 2010, Dorahy & Kannis-Dymand 2012). Unreinforced masonry commercial and office buildings in the two business districts performed poorly, with two buildings collapsing and many partially collapsed, which would have led to numerous deaths and injuries had the buildings been occupied (Wood et al. 2010).
The immediate emergency response to the earthquake was effective, with local authorities, lifeline utility operators, engineers and national agencies responding using planned arrangements. While outages occurred, power and telecommunications were restored to 90 per cent within 24 hours, with water supplies restored within five days (Wood et al. 2010). Despite the small number of injuries and swift emergency response, residents of areas most affected by the earthquake were more likely to report depression and anxiety symptoms. This was due to stress and sleep disruption, which may be explained by property damage, increased fatigue and uncertainty about the future, including further aftershocks (Kemp et al. 2011, Dorahy & Kannis-Dymand 2012).
The following year a 6.3 magnitude earthquake occurred at 12:51pm on 22 February 2011 in Christchurch (Doocy et al. 2013). The earthquake resulted in 185 fatalities, 6 659 injuries and widespread damage to buildings and infrastructure, particularly in the central business district (Giovinazzi et al. 2011, Ardagh et al. 2012, Sibley & Bulbulia 2012). The collapse of two multi-storey office buildings and associated fires led to 110 fatalities. Falling debris crushed two buses, killing six individuals, with another 16 dying from falling debris and landslides (Sibley & Bulbulia 2012). While the majority of injuries were minor, serious injuries occurred as a result of falls and being struck by rubble. Patients who were trapped under rubble suffered crush syndrome, characterised by severe shock and renal failure following crushing trauma to skeletal muscle. Soft tissue injuries and bone fractures were common (Ardagh et al. 2012). Emergency services were overwhelmed, hospitals exceeded their capacity, power, water and telecommunications outages were extensive and prolonged and many residents were displaced (Sibley & Bulbulia 2012).
Christchurch has one hospital with an emergency department, which is located on the edge of the central business district. It sustained significant damage, including loss of power, emergency generator failure, and collapse of a section of the ambulance bay. Damage to roads and communications failures contributed to difficulties in triage of patients. However, the hospital activated its well-developed and annually rehearsed incident plans, which ensured that staff were effectively managed, patients were identified using pre-labelled packs and wards were equipped with torches, headlamps and charged batteries. Thus, although the earthquake occurred during the day when many people were in high-rise concrete buildings and there were two full multi-storey building collapses, Christchurch’s stringent building codes and the proximity to high quality and well-managed healthcare minimised fatalities (Ardagh et al. 2012).

Image: Printed with permission from Stuff.co.nz
Patients and staff outside the emergency department at the Christchurch Hospital.
United States of America
The 1989 Loma Prieta and the 1994 Northridge earthquakes in California highlight the potential for road destruction during earthquakes. The Loma Prieta earthquake occurred in Santa Clara County in Northern California on 17 October 1989 at 5:04pm and registered 7.1 on the Richter scale (Pointer et al. 1992). The earthquake caused 63 fatalities and 3 757 injuries, with 42 deaths among motor vehicle occupants and pedestrians resulting from the partial collapse of an elevated freeway ramp (Pointer et al. 1992). The earthquake occurred when many residents were in their homes preparing to watch a World Series baseball match, leaving the usually heavily congested freeways relatively quiet. Had this not been the case, the fatality and injury rates would have been much higher. Furthermore, two large sections of the San Francisco-Oakland Bay Bridge fell, resulting in one fatality and rendering the bridge unusable. Damage to 18 306 residential properties and 2 575 businesses resulted in the displacement of 12 053 people (Nolen-Hoeksema & Morrow 1991, Pointer et al. 1992).
The most common injuries sustained during the Loma Prieta earthquake included falls, cuts, abrasions, fractures, burns and being hit by falling objects. While five local hospitals reported difficulties in treating patients due to staffing shortages and insufficient operating suites, most hospital resources were not overwhelmed. Although hospitals near the epicentre experienced a near doubling in the number of patients presenting to the emergency department, off-duty doctors and nurses were able to deal with the influx. The familiarity with and preparation for earthquakes in the region resulted in rapid triaging and expedited paperwork, ensuring that the earthquake did not impact negatively on patient care (Pointer et al. 1992).
The 1994 magnitude 6.7 Northridge earthquake occurred on 17 January 1994 at 4:31am in the San Fernando Valley of Los Angeles (Scientists of the US Geological Survey and the Southern California Earthquake Center 1994, Bolin & Stanford 1998, Peek-Asa et al. 1998, Knight et al. 2000). The damage was widespread, including fires, downed power lines and traffic signals, and property and road damage. Over 12 000 residential properties, businesses and hospitals sustained structural damage, leading to the displacement of over 20 000 residents. Schools experienced substantial non-structural damage such as falling lights, which would have resulted in fatalities had schools been in session. Disruptions continued for months due to damaging aftershocks and the collapse of freeway overpasses, which resulted in three major freeways remaining closed until they were rebuilt. However, the emergency response to the earthquake was efficient and preparations such as the retrofitting of masonry buildings prevented more widespread damage (Scientists of the US Geological Survey and the Southern California Earthquake Center 1994).
The earthquake resulted in 57 fatalities that were mostly due to building collapse leading to asphyxia and crush syndrome. Over 7 000 injuries required hospitalisation that were primarily due to falls or being hit by objects (Peek-Asa et al. 1998, 2000). Older individuals were more likely to be injured due to their decreased ability to move quickly to avoid falling debris and their lower tolerance to sustained injuries (Mahue-Giangreco et al. 2001). However, older individuals displayed the lowest levels of earthquake-specific negative thought patterns and those with prior exposure to earthquakes were less likely to experience post-earthquake depression (Knight et al. 2000).
Recommendations
Some work has already been done or is underway in South Australia that addresses the damage that could occur during an earthquake. An earthquake hazard mapping exercise has identified the areas of South Australia most likely to experience an earthquake and estimated the numbers of fatalities and injuries that would occur during earthquakes of various magnitudes and epicentre locations. However, more can be done to expand on existing knowledge in order to improve South Australia’s preparedness.
Currently, there are no sufficiently strong motion recorders installed in South Australia to determine the manner in which the earth might shake during an earthquake (McCue 2010). It is not clear whether the movement would be different to earthquakes occurring in relatively similar locations. While the absence of these data leads to difficulties in predicting the impact that an earthquake of a given magnitude would have on existing structures, there are nonetheless important recommendations for Adelaide that can be drawn from the events reported on in this article. Key recommendations are summarised in Table 2.
Table 2: Key recommendations
|
Area |
Recommendations |
|
Building standards |
|
|
Transport and infrastructure |
|
|
Community preparedness |
|
|
Health services |
|
|
Recovery and rehabilitation |
|
|
Practical and financial support |
|
Considering the damage sustained by unreinforced masonry buildings during previous earthquakes, it has been argued that the most significant earthquake risk mitigation in South Australia will be through improving building standards (Ramirez & Peek-Asa 2005, Gibson 2010). Some areas of Adelaide, particularly the inner-city and eastern suburbs, have buildings of similar age and construction to Christchurch, with substantial numbers of unreinforced masonry buildings. Due to the high level of earthquake hazard in New Zealand unreinforced masonry buildings have been seismically assessed and retrofitted where necessary, with most retrofitted buildings performing well during the 2010 Christchurch earthquake (Wood et al. 2010). Following the Adelaide and Newcastle earthquakes a number of school buildings in Adelaide and Newcastle were strengthened and a hospital in Adelaide was relocated away from what was thought to be an active fault in the southern suburbs (McCue 2010). It may be necessary to assess the economic viability of retrofitting unreinforced masonry buildings in Adelaide that may lead to high numbers of fatalities and injuries during an earthquake (Greenhalgh et al. 1994).
Bridges and roads are highly vulnerable to earthquake damage, resulting in numerous injuries and fatalities (Nolen-Hoeksema & Morrow 1991, Marmar et al. 1996, Peek-Asa et al. 1998, Ramirez & Peek-Asa 2005). Many bridges in South Australia are relatively old and therefore may be prone to cracking in the event of an earthquake (Templeman & Bergin 2008). The failure of infrastructure, such as traffic signals and road lighting, may also contribute to accidents and injuries (Ramirez & Peek-Asa 2005). Damaged roads and bridges may make it difficult to access essential services, including hospitals (Ardagh et al. 2012). Thus, alternate routes or modes of transport should be part of emergency plans.
The importance of each community’s level of preparation must be acknowledged. Research has demonstrated that social capital, or the degree of trust and connection between community members, is a strong predictor of post-disaster recovery. Communities should focus on developing social infrastructure, such as community networks and organisations, which contribute to greater resilience and rapid recovery (Aldrich 2010). Communities should develop knowledge and understanding of earthquakes and ensure the availability of essential supplies, transport and communications services (Templeman & Bergin 2008, Gibson 2010). Essential services, including hospitals, should have sound emergency power and communications systems and contingency plans in place. Emergency operation plans should be developed and rehearsed, including well-defined hierarchical structures for the management of staff and volunteers (Ardagh et al. 2012). In the event of a large earthquake, it is likely a national (and potentially international) response will be required during the response and recovery period (Templeman & Bergin 2008). Arrangements should be in place to enable effective co-ordination and communication between local and national service providers and for the endorsement and co-ordination of international disaster response teams.
The South Australia Department for Manufacturing, Innovation, Trade, Resources and Energy (Mineral Resources Division) manages earthquake monitoring devices in South Australia. Sites include Government House, Mt Osmond, Whyalla, Port Pirie, Napperby, Payneham, and Torrens Island. The stations are moved around the metropolitan area every two years.

Image: South Australia Department for Manufacturing, Innovation,
Trade, Resources and Energy
Early trigger earthquake recorder used in metropolitan areas of South Australia.
Health services should be prepared to deal with the pattern of injuries routinely observed during earthquakes, including crush syndrome, soft tissue injuries and bone fractures (Ardagh et al. 2012, Doocy et al. 2013). Acute kidney injury is common in patients with crush syndrome and rapid provision of renal replacement therapy is important. Injured individuals are likely to attend the closest or most familiar health facility in the event of an earthquake and may present to facilities that would not normally receive seriously injured patients. Thus, robust emergency plans should be in place for all healthcare providers, not only major hospitals. Moreover, the state health system’s capacity to manage a large mass casualty event needs to be maintained and practiced and plans put in place to collaborate effectively with national and international health agencies (Templeman & Bergin 2008).
Longer-term recovery and rehabilitation should be considered, not only in regard to physical trauma, but also taking psychological impacts into account. Although psychological problems among earthquake survivors decline substantially over time, a minority continue to experience significant and persistent mental illness (Lewin et al. 1998). It is important that these individuals be able to access treatment and support services, not only immediately after the disaster, but throughout their recovery period. Those with elevated levels of depression and stress prior to an earthquake and a ruminative style of responding to these symptoms may benefit from engagement in relief efforts and other similar activities that have a positive influence on their sense of efficacy and overall mental state (Nolen-Hoeksema & Morrow 1991).
Earthquakes have ongoing and substantial effects on the lives of individuals and local businesses, rather than being events with a well-defined endpoint. Thus, it is important to recognise that sole reliance on initial earthquake exposure to identify individuals in need of support will exclude those for whom the impact is latent, occurring as a result of accumulation of ongoing disruptions and resulting stress. In order to decrease these disruptions, prompt repairs, speedy settlement of insurance claims, financial assistance and flexible employment arrangements should be made available to individuals and businesses affected by earthquake (Carr et al. 1997).
The level of preparation for an earthquake event and the characteristics of the impact, such as fatality and injury rates and damage to essential services, may be underestimated when the Adelaide context is compared in a crude fashion to the experiences of similar cities. The engagement of civil society through community awareness and preparedness is influenced by the community’s recent experiences of disaster. In Adelaide, where significant earthquakes are infrequent, an earthquake may have a greater impact because the community, its public policy, organisations and individual community members, are less aware of the potential risks.
References
Aldrich, DP 2010, The power of people: social capital’s role in recovery from the 1995 Kobe Earthquake. Natural Hazards. doi: 10.1007/s11069-101-9577-7.
Ardagh, MW, Richardson, SK, Robinson, V, Than, M, Gee, P, Henderson, S, Khodaversi, L. Mckie, J. Robertson, G, Schroeder PP & Deely, JM 2012, The initial health-system response to the earthquake in Christchurch, New Zealand, in Ferbuary, 2011. The Lancet 379: pp. 2109-2115.
Bolin, R & Stanford, L 1998, The Northridge earthquake: community-based approaches to unmet recovery needs. Disasters 22(1): pp. 21-38.
Carr, VJ, Lewin, TJ, Kenardy, JA, Webster, RA, Hazell, PL, Carter, GL & Williamson, M 1997, Psychosocial sequelae of the 1989 Newcastle earthquake: III. Role of vulnerability factors in post-disaster morbidity. Psychological Medicine 27: pp. 179-190.
Carr, VJ, Lewin, TJ, Webster, RA & Kenardy, JA 1997, A synthesis of the findings from the Quake Impact Study: a two-year investigation of the psychosocial sequelae of the 1989 Newcastle earthquake. Soc Psychiatry Psychiatr Epidemiol 32: pp. 123-136.
Carr, VJ, Lewin, TJ, Webster, RA Kenardy, JA, Hazel, PL & Carter, GL 1997, Psychosocial sequelae of the 1989 Newcastle earthquake: II. Exposure and morbidity profiles during the first 2 years post-disaster. Psychological Medicine 27: pp. 167-178.
Doocy, S, Daniels, A, Packer, C, Dick, A & Kirsch, TD 2013, The human impact of earthquakes: a historical review of events 1980-2009 and systematic literature review. PLoS Currents 5: ecurrents.dis.67bd14fe457f451db450b5433a5438ee5420fb5833.
Dorahy, MJ & Kannis-Dymand, L 2012, Psychological distress following the 2010 Christchurch earthquake: a community assessment of two differentially affected suburbs. Journal of Loss and Trauma 17: pp. 203-217.
Doyle, HA, Everingham, IB & Sutton, DJ 1968, Seismicity of the Australian continent. Journal of the Geological Society of Australia: An International Geoscience Journal of the Geological Society of Australia 15(2): pp. 295-312.
Gibson, G 2010, Earthquake risk in Australia. Australian Planner 47(1): pp. 54-57.
Giovinazzi, S, Wilson, T, Davis, C, Bristow, D, Gallagher, M, Schofield, A, Villemure, M, Eidinger, J & Tang, A 2011, Lifelines performance and management following the 22 February 2011 Christchurch earthquake, New Zealand: highlights of resilience. Bulletin of the New Zealand Society for Earthquake Engineering 44(4): pp. 402-417.
Greenhalgh, SA, Love, D, Malpas, K & McDougall, R 1994, South Australian earthquakes, 1980-92. Australian Journal of Earth Sciences: An International Geoscience Journal of the Geological Society of Australia 41(5): pp. 483-495.
Kemp, S, Helton, WS, Richardson, JJ, Blampied, NM & Grimshaw, M 2011, Sleeplessness, stress, cognitive disruption and academic performance following the September 4, 2010, Christchurch earthquake. Australasian Journal of Disaster and Trauma Studies 2011-2012: pp. 11-18.
Knight, BG, Gatz, M, Heller, K & Bengtson, VL 2000, Age and emotional response to the Northridge earthquake: a longitudinal analysis. Psychology and Aging 15(4): pp. 627-634.
Lewin, TJ, Carr, VJ & Webster, RA 1998, Recovery from post-earthquake psychological morbidity: who suffers and who recovers? Australian and New Zealand Journal of Psychiatry 32: pp. 15-20.
Mahue-Giangreco, M, Mack, W, Seligson, H & Bourque, BL 2001, Risk factors associated with moderate and serious injuries attributable to the 1994 Northridge earthquake, Los Angeles, California. Annals of Epidemiology 11: pp. 347-357.
Marmar, CR, Weiss, DS, Metzler, TJ, Ronfeldt, HM & Foreman, C 1996, Stress responses of emergency services personnel to the Loma Prieta earthquake interstate 880 freeway collapse and control traumatic incidents. Journal of Traumatic Stress 9(1): pp. 63-85.
McCue, K 2010, Assessing earthquake hazard and risk in Australia. Australian Planner 47(1): pp. 52-53.
Nolen-Hoeksema, S & Morrow, J 1991, A prospective study of depression and posttraumatic stress symptoms after a natural disaster: the 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology 61(1): pp. 115-121.
Peek-Asa, C, Kraus, JF, Bourque, LB, Vimalachandra, V, Yu, J & Abrams, J 1998, Fatal and hospitalized injuries resulting from the 1994 Northridge earthquake. International Journal of Epidemiology 27: pp. 459-465.
Peek-Asa, C, Ramirez, M, Shoaf, K, Seligson, H & Kraus, JF 2000, GIS mapping of earthquake-related deaths and hospital admissions from the 1994 Northridge, California earthquake. Annals of Epidemiology 10(1): pp. 5-13.
Pointer, JE, Michaelis, J, Saunders, C, Martchenke, J, Barton, C, Palafox, J, Kleinrock, M & Calabro, JJ 1992, The 1989 Loma Prieta earthquake: impact on hospital patient care. Annals of Emergency Medicine 21(10): pp. 1228-1233.
Ramirez, M & Peek-Asa, C 2005, Epidemiology of traumatic injuries from earthquakes. Epidemiologic Reviews 27: pp. 47-55.
Scientists of the US Geological Survey and the Southern California Earthquake Center 1994, The maginitude 6.7 Northridge, California, earthquake of 17 January 1994. Science 266: pp. 389-397.
Sibley, CG & Bulbulia, J 2012, Faith after an earthquake: a longitudinal study of religion and perceived health before and after the 2011 Christchurch New Zealand earthquake. PLoS ONE 7(12): e49648.
State Emergency Management Committee 2012, State Emergency Management Plan. Adelaide, Government of South Australia.
Sutton, DJ & White, RE 1968, The seismicity of South Australia. Journal of the Geological Society of Australia: An International Geoscience Journal of the Geological Society of Australia 15(1): pp. 25-32.
Templeman, D & Bergin, A 2008, Taking a punch: building a more resilient Australia. Canberra, Australian Strategic Policy Institute.
Wood, P, Robins, P & Hare, J 2010, Preliminary observations of the 2010 Darfield (Canterbury) earthquakes: an introduction. Bulletin of the New Zealand Society for Earthquake Engineering 43(4): pp. i-iv.
World Association for Disaster and Emergency Medicine 2003, Health Disaster Management: Guidelines for Evaluation and Research. Madison, WADEM.
About the authors
Dr Olga Anikeeva is a Postdoctoral Research Fellow at Torrens Resilience Institute and the Disaster Research Centre at Flinders University with a background in public health and epidemiology.
Dr Malinda Steenkamp is a Postdoctoral Research Fellow at Torrens Resilience Institute and the Disaster Research Centre at Flinders University. She has a background in epidemiology, public health and maternal and infant health.
Professor Paul Arbon is the Director of Torrens Resilience Institute and the Disaster Research Centre at Flinders University and current President of the World Association for Disaster and Emergency Medicine. His research focuses on disaster resilience and the health aspects of disaster response and recovery.