Abstract
Natural disasters are growing in intensity and frequency worldwide, effecting over 1.5 billion people in the past decade. Individuals with a disability are at greater risk of injury and death than are other populations. Individuals with disabilities often have specific needs leading to difficulties when seeking shelter during disaster events. Emergency shelters are generally not purposefully built to accommodate such requirements. To assess the extent of this, a review was undertaken to synthesise current literature on the experience of individuals with disabilities in emergency shelters and to identify gaps to inform future research. Initial searches identified 185 articles and six studies were included in the review. Synthesis of study findings highlighted context-specific factors of emergency shelter experiences on individuals with disabilities during natural disasters. These factors were the physical, social and attitudinal environments. Quaill and colleagues (2018) reported the need for meaningful engagement with individuals with disabilities in disaster planning broadly. This paper identifies the importance disability inclusive risk reduction specific to shelter planning to allow for safety and maintenance of independence. The small body of research identified indicates that this aspect is under-researched in Australia as well as internationally. This has implications for the understanding of disaster risk reduction requirements for individuals with a disability.
Introduction
Natural disasters are increasing in intensity and frequency (Thomas & López 2015). Individuals with a disability make up approximately 15 per cent of the world’s population and are at greater risk and experience higher mortality rates and poorer disaster recovery outcomes after disasters (Quaill, Barker & West 2018, World Health Organization 2011). This is exacerbated by increased strain on support networks during natural disasters and social stigma towards vulnerable populations. These factors influence their access to evacuation, shelter and relief supplies (Howard et al. 2017, Gorman-Murray et al. 2018).
Emergency shelters are established in a variety of settings, including public buildings and temporary structures. The term ‘emergency shelter’ refers to temporary places of refuge during all phases of an emergency event. In Queensland, emergency shelter definitions include immediate shelters (used for 1–18 hours), temporary shelters (used in excess of 18 hours and up to several weeks) and temporary housing (longer-term temporary accommodation that facilitates transition to permanent living situations) (Queensland Government 2018). This study revealed that there is no internationally standardised terminology for shelter types and shelter definitions differ across regions and countries.
During all phases of a disaster, people evacuating their homes should be in a safe and accessible environment that is equipped to meet their needs. Individuals with disabilities often have specific needs including accessibility, specialised equipment, medication storage and support from trained health care workers (Gorman-Murray et al. 2018, Twigg et al. 2011, Ochi, Murray & Hodgson 2013). However, emergency shelters are often not purposefully planned or built to accommodate these requirements.
The Sendai Framework for Disaster Risk Reduction 2015–2030 (United Nations Office for Disaster Risk Reduction 2015) is the first international disaster risk reduction agreement to address the needs of individuals with disabilities. Understanding of disaster risk, including vulnerability and environmental impacts, is one of the four priorities for action outlined in the framework. In addition, the framework identifies that engagement with individuals with a disability is pivotal to the formulation of inclusive and effective disaster planning. The framework acknowledges the context-specific needs of individuals with disabilities during disasters and promotes universal access to evacuation vehicles, resources and emergency shelters.
Aim
Globally, few studies have examined the experiences of individuals with disabilities in emergency shelters. The aim of this review was to synthesise current literature in this area and to identify gaps in current knowledge to inform future research.
The specific research question was: ‘What factors have influenced the experience of individuals with disabilities in emergency shelters during natural disasters?’
Method
The literature review was conducted using an integrative approach to facilitate synthesis of diverse research methodologies (Whittemore & Knafl 2005). A systematic search was conducted using keyword terms and phrases of ‘natural disasters’, ‘disaster planning’, ‘disability’, ‘disabled’, ‘evacuation centre’, ‘shelters’, ‘rest centres’ and ‘emergency shelter’ in various combinations. Databases searched included Medline (Ovid), CINAHL, PsycINFO and Scopus. The search was limited to peer-reviewed publications between 1998 and 2018. This period was selected as it represents an era during which significant disaster management reforms occurred, particularly in response to Hurricane Katrina in 2005 (Brodie et al. 2006, Centers for Disease and Prevention 2006). Articles included relate to the experience of individuals with a disability in emergency shelters prior to, during and following a natural disaster.
A total of 185 articles was identified during the initial search. These were screened for inclusion according to the PRISMA1 flow diagram (see Figure 1) by two independent reviewers (Moher et al. 2009). Six studies were included for review and were appraised for quality using the Critical Appraisal Skills Programme appraisal tool (2017).
Results
The six studies comprised four qualitative studies, one mixed-methods study and one narrative review. Data collection methods of these publications included semi-structured interviews (n=4), a survey questionnaire (n=1) and a synthesis of grey and published literature (n=1). Included studies investigated emergency shelter experiences from a range of natural disasters (earthquakes, floods, tsunamis and cyclones) and shelter structures (health care centres, schools, shipping containers, leisure centres, tents and shrines). Examples were from Japan, Iran, the USA and the United Kingdom. Participants included individuals with physical, psychosocial and age-related disabilities (Aryankhesal, Pakjouei & Kamali 2017, Maeda, Shamoto & Furuya 2017, Missildine et al. 2009). Four studies did not specify the disability of participants but did detail the functional impact of the participants’ disability, for example wheelchair use and reduced mobility (Brittingham & Wachtendorf, 2013, Kipling et al. 2011, Maeda, Shamoto & Furuya 2017, Twigg et al. 2011).
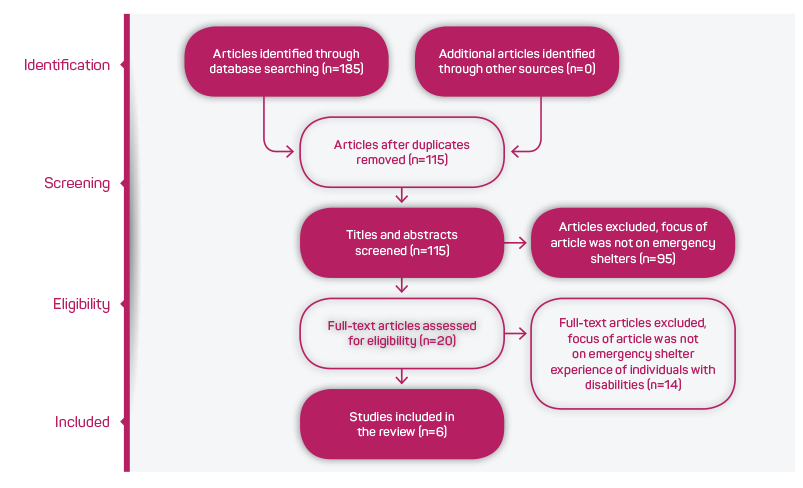
Figure 1: PRISMA flow diagram of papers selected for this study. Source: Adapted from Moher et al. 2009
Methodological quality varied across the studies. Five studies used observational and narrative designs, often with broad research questions, limiting the generalisation of findings to the wider population. Three studies did not specify participant numbers or demographics, limiting the contextualisation of data collected (Brittingham & Wachtendorf 2013, Maeda, Shamoto & Furuya. 2017, Twigg et al. 2011). Four of the studies involved interviewing participants after six months and up to 25 years following the disaster event. This raises the possibility of recall bias (Aryankhesal, Pakjouei & Kamali 2017, Brittingham & Wachtendorf 2013, Kipling, Newton & Ormerod 2011, Twigg et al. 2011). Conversely, the findings of two studies, conducted with evacuees shortly after or during the disaster by shelter staff who continued to support their needs, may have led to respondent bias or perceived coercion (Missildine et al. 2009, Maeda, Shamoto & Furuya 2017).
A summary of the articles reviewed is presented in Table 1.
People’s experiences of emergency shelters varied according to the context of the disaster (e.g. Japan versus USA) and type of disaster (earthquake versus hurricane). Across the six studies, three themes emerged as factors influencing the experiences of emergency shelters for individuals with a disability:
- Physical environment (e.g. natural environment, human-made environmental changes and technology).
- Social environment (e.g. support, communication, relationships and social services).
- Attitudinal environment (e.g. culture, norms and ideology).
These themes are consistent with the definitions of ‘Environmental Factors’ within the World Health Organization International Classification of Functioning, Disability and Health2 framework for measuring health and disability.
Influence of the physical environment
Individuals with a disability can have an enhanced or worsened experience of an emergency shelter depending on the physical environment. Newer and public buildings constructed to building codes were more disability inclusive and facilitated in the independence of evacuees and reduced their risk of poor health outcomes (Kipling, Newton & Ormerod 2011, Twigg et al. 2011). Temporary structures such as tents increased the risk of injury and death for individuals with a disability; secondary to extreme temperatures, vermin infestation and fire (Aryankhesal, Pakjouei & Kamali 2017).
Emergency shelters with accessible toilets supported the independence for individuals with reduced mobility. Shelters with no toilet facilities or disability exclusive toilet facilities (e.g. tents, older buildings with unmodified bathrooms, Japanese-style toilets) resulted in perceptions of loss of dignity for individuals with disabilities (Aryankhesal, Pakjouei & Kamali 2017, Brittingham & Wachtendorf 2013, Kipling, Newton & Ormerod 2011, Maeda, Shamoto & Furuya 2017, Twigg et al. 2011). The risk of poor health outcomes due to a lack of appropriate bathroom facilities was exacerbated by extended periods using temporary shelters and housing, with some used by evacuees for many months.
Sleep was significantly affected with five studies reporting that the lack of appropriate bedding could disturb sleep and threaten the health and independence of individuals with a disability. Cots or mattresses on the floor did not provide adequate body pressure relief for individuals who are unable to move independently. This increased the need for physical assistance to get in and out of bed. Consequently, poor recovery health outcomes resulted for some individuals, including pressure injuries (Missildine et al. 2009, Brittingham & Wachtendorf 2013, Maeda, Shamoto & Furuya 2017, Twigg et al. 2011, Aryankhesal, Pakjouei & Kamali 2017).
Space limitations in a crowded shelter environment presented significant threats to the independence of individuals using specialised equipment such as wheelchairs (Brittingham & Wachtendorf 2013, Maeda, Shamoto & Furuya 2017, Missildine et al. 2009). Restricted space meant evacuees with a disability were unable to move about without physical assistance from family or carers. Where emergency shelters had been specifically designated for use by individuals with disabilities, often a larger space was allocated to facilitate use of specialist equipment. Three studies identified that demarcation of allocated space using screens or floor outlining enhanced privacy, facilitated use of mobility devices and reduced the risk of space being encroached upon by others (Brittingham & Wachtendorf 2013, Missildine et al. 2009, Kipling, Newton & Ormerod 2011).
Influence of the social environment
Providing up-to-date information in emergency shelters is important for the safety, health and independence of evacuees who have augmented communication needs. Lack of accessible communication methods (e.g. hearing loops, braille) could result in safety warnings being missed and shelter services not being accessed. In shelters without these communication options, evacuees with a disability reported being unaware of the availability of supplies such as food and blankets (Brittingham & Wachtendorf 2013, Kipling, Newton & Ormerod 2011). Inaccessibility of information was not limited to individuals with visual or hearing impairments. Individuals with reduced mobility reported being unaware of information displayed in communal areas where they could not use walking aids in confined spaces (Brittingham & Wachtendorf 2013, Maeda, Shamoto & Furuya 2017).
Training of staff and volunteers varied significantly across the included studies depending on geographical location, natural disaster and shelter type. Personnel working in shelters specifically designated for use by individuals with special needs were more likely to have received training to support the independence of people with disabilities (Brittingham & Wachtendorf 2013, Maeda, Shamoto & Furuya 2017, Missildine et al. 2009). However, one study from Japan identified that training and enthusiasm varied across shelter staff, even within dedicated special-needs shelters (Brittingham & Wachtendorf 2013). Lack of appropriate training in the provision of physical assistance and management of mental health conditions increased the risk of injury to both evacuees with disabilities and to shelter personnel (Brittingham & Wachtendorf 2013, Kipling, Newton & Ormerod 2011). The burden of care on shelter personnel was amplified by evacuees being separated from their carers, families or assistance animals (e.g. guide dogs). This was due to overcrowding and implementation of disability exclusive emergency shelter policy (Brittingham & Wachtendorf 2013, Twigg et al. 2011).
| Title/Author/Year | Research Design | Participants | Summary of findings |
|
Safety Needs of People With Disabilities During Earthquakes. Aryankhesal, Pakjouei & Kamali 2017. |
Qualitative semi-structured interviews. | Twelve people with disabilities and experience of earthquakes in Iran (Roodbar-Manjil in 1990, Avaj in 2002, Bam in 2003 Firoozabad-Kojour in 2004, Varzeqn-Ahar in 2012). | Shipping containers with basic amenities were more suitable shelters for individuals with disabilities than tents due to better accessibility and temperature control. Tent shelters exposed evacuees to extreme temperature changes, vermin and insect infestation, vulnerability to fire and lack of bathroom amenities. |
|
The Effect of Situated Access on People with Disabilities: An Examination of Sheltering and Temporary Housing after the 2011 Japan Earthquake and Tsunami. Brittingham & Wachtendorf 2013 |
Qualitative interviews 3–6 months post-disaster. | Shelter users with a disability after the 2011 Tohoku-oki earthquake and tsunami in Japan. Sample size and demographics not specified. |
Japanese-style toilets were unsuitable for individuals with a disability due to the physical assistance required. The lack of training for volunteers and shelter staff in ‘social welfare’ shelters (for individuals with special needs) impacted on the quality of care. In Japan, the stigma associated with having a disability affects planning and resourcing of ‘social welfare’ shelters. It also influences the behaviour of other shelter residents towards evacuees with disabilities in shelters. |
|
Accessing emergency rest centres in the UK - lessons learnt. Kipling, Newton & Ormerod 2011. |
Qualitative, semi-structured interviews 5–6 months post-disaster. |
Nine members of a shelter administration team during the flooding of the Yorkshire and Humber regions of the United Kingdom in 2007, including managers, volunteers (one volunteer with a disability). |
Heritage listed buildings had limited bathroom accessibility and wheelchair users had to get physical assistance to access them. Recently refurbished buildings had accessible toilets, lowered counters and automated doors. Showers had no seating nor rails installed, impacting on the personal hygiene of wheelchair users living in the shelter for many weeks. Shelters had limited enhancements to assist individuals who were deaf of hearing impaired and had no braille information. The limited training of shelter volunteers impacted on the care of evacuees with mental health conditions. |
|
Feeding Support Team for Frail, Disabled, or Elderly People during the Early Phase of a Disaster. Maeda, Shamoto & Furuya 2017. |
Mixed-method study comprising qualitative, semi-structured interviews and statistical analysis of quantitative health outcome data. |
Shelter users following the Kumamoto earthquake in 2016 in Japan who identified as frail, disabled or elderly. Sample size and demographics not specified. |
Evacuees reported a reluctance to use bathrooms due to overcrowding and poor bathroom facilities. Discrimination towards individuals with a disability in Japan impacted on the equity of resources. Shelter users with a disability were susceptible to dehydration due to reduced water consumption secondary to mobility and staffing levels. |
|
Comfort in the Eye of the Storm: A Survey of Evacuees with Special Medical Needs. Missildine, Varnell, Williams, Grover, Ballard & Stanley-Hermanns 2009. |
Descriptive study using qualitative surveys on day four of evacuation. | Eighty-two participants in ‘special medical needs’ shelter in Texas, USA following Hurricane Gustav in in 2008. | Evacuees felt reassured by the presence of medically trained staff. Improvements suggested were better access to bathroom facilities, greater variety of food and increased provision of activity programs and exercise |
|
Disability and public shelter in emergencies. Twigg, Kett, Bottomley, Tan & Nasreddin 2011. |
Narrative review of peer-reviewed, grey and policy literature on experiences of people with disabilities in public shelters during emergencies. | Review of government reports (n=26), policy documents (n=14), peer-reviewed studies (n=9) and unpublished works (n=4) following Hurricane Katrina in the USA in 2005, the West Bengal cyclone in Bangladesh in 2002 and the Indian Ocean tsunami in 2004. |
Registration and assessment procedures failed to identify individuals with disabilities and special needs; particularly functional needs. Evacuees with a disability experienced refusal of admission to shelters on grounds that shelters cannot manage a person’s disability, particularly mental health conditions. Family members and carers of individuals with a disability were discouraged from accompanying them due to overcrowding. Communication methods were problematic due to a lack of hearing loops and systems or braille. Cultural constraints restricted women with a disability from using bathroom facilities. |
Influence of the attitudinal environment
Attitudes of community members and people in positions of authority can significantly impact on the experiences of individuals with disabilities requiring shelter during and in the aftermath of disasters. Stigma associated with disability in the Japanese context was perceived to create inequity of access to shelter supplies and services. In shelters for the general population, individuals with a disability reported experiencing hostility from other evacuees related to the additional space allocated for the use of mobility devices (Brittingham & Wachtendorf 2013, Maeda, Shamoto & Furuya 2017). A thorough understanding of context-specific attitudinal and cultural environment to inform disaster risk reduction for individuals with disabilities is required.
Cultural practices in relation to physical assistance could result in increased risk to the safety of individuals with disabilities in some cultures. In Japan, evacuees were likely to refuse assistance for activities involving the removal of clothing to go to the toilet. This increased the risks of falls and affected personal hygiene (Brittingham & Wachtendorf 2013). This reluctance to accept assistance resulted in people voluntarily restricting their food and water intake to reduce the need for toileting and avoid the feelings of shame and loss of dignity (Brittingham & Wachtendorf 2013, Maeda, Shamoto & Furuya 2017). In Bangladesh, cultural and religious practices restricted the use of bathrooms by women with a disability. These restrictions increased the likelihood of these women leaving shelters prematurely and being exposed to greater risk of injury or death (Twigg et al. 2011).
Discussion
These findings indicate that experiences of individuals with a disability using emergency shelters are influenced by the physical, social and attitudinal factors that can affect health, safety and independence. Individuals with a disability are the most appropriate source of advice regarding the potential threats to their safety and independence in the event of a natural disaster (Kipling, Newton & Ormerod 2011, Twigg et al. 2011). Despite the promotion of the involvement of individuals with disabilities in disaster risk reduction by the United Nations Office for Disaster Risk Reduction, this review showed there is limited research documenting this. Experiences of individuals with a disability accessing and using emergency shelters is limited compared with reports from service providers such as shelter personnel, non-government organisation workers and local government officials.
Variation in experiences in different countries and different types of disasters suggests that context-specific emergency shelter planning is essential for the health and functional needs of individuals with disabilities. For example, cyclones, bushfires and floods occur frequently in Australia and often necessitate evacuation of community members to emergency shelters. To date, no studies have been undertaken in Australia to investigate factors influencing emergency shelter experiences from the perspective of individuals with disabilities. Future research needs to include meaningful engagement with individuals with a disability at the local level to address any barriers to safety and independence. Exploration of such experiences will allow a strong voice for individuals with disabilities to advocate for culturally appropriate, disability inclusive emergency shelter facilities by local governments and service providers.
Individuals with disabilities comprise up to 15 per cent of the world’s population. However, in the event of natural disaster there are limited physical and human resources dedicated to meeting their specific needs (World Health Organization 2011, Quaill, Baker & West 2018). The experiences of individuals with a disability in disaster situations are varied and disparity is influenced by diagnoses, support networks available and the application of a one-size-fits-all approach to establish special-needs emergency shelters (Kipling, Newton & Ormerod 2011). A functional and needs-based strategy by emergency management planners, rather than a disability focused approach, may be more appropriate to meet the needs of individuals with disabilities in emergency shelters (Twigg et al. 2011, Fannin et al. 2015).
Limitations
This review comprised a small number of studies from a wide variety of disciplines including heterogeneity of population, disaster types and cultural contexts. It is possible that studies related to this field were missed despite extensive and systematic search. Studies used in this review were assessed as being of low to moderate methodological quality and, while relevant to include, findings should be interpreted with caution.
Conclusion
The experience of individuals with a disability using emergency shelters is under-researched. This limits the understanding of their requirements and the strategies needed for this population from government agencies, disaster planners and the wider community. This review reveals the context-specific nature of the shelter experience and the added effects of the physical, social and attitudinal environments. This complexity reinforces the need for meaningful engagement with individuals with a disability in emergency management planning to meet the range of functional needs and reduce risk for this population. In Australia, the narrative is yet to be explored of the experiences of individuals with disabilities who use emergency shelters, including personal factors, barriers and enablers. Further research in this area will assist emergency management policy and protocol formulation that is truly inclusive and is informed by the needs of individuals with a disability in emergency shelter environments.
Footnotes
- A PRISMA flow diagram is a graphical representation of the flow of citations reviewed in the course of a systematic review.