Moving from theory to praxis on the fly: Introducing a salutogenic method to expedite mental health care provision in disaster situations
Jan Golembiewski
By, J A Golembiewski BfA, BArchS, March, PhD Scholar, Architecture, Planning and Design, University of Sydney
Article
(Originally presented at the Australian Rural and Remote Mental Health Symposium in Canberra, 2 November 2009)
Introduction
Not a lot is known about most mental illness. Its triggers can rarely be established and nor can its aetiological dynamics, so it is hardly surprising that the accepted treatments for most mental illnesses are really strategies to manage the most overt symptoms. But with such a dearth of knowledge, how can worthy decisions be made about psychiatric interventions, especially given time and budgetary restrictions?
This paper introduces a method, extrapolated from Salutogenics; the psycho-social theory of health introduced by Antonovsky in 1987. This method takes a normative stance (that psychiatric health care is for the betterment of psychiatric patients), and applies it to any context where there is a dearth of workable knowledge. In lieu of guiding evidence, the method identifies reasonable alternatives on the fly, enabling rational decisions to be made quickly with limited resources.
An emergency psychiatric response is the sort of time-critical intervention that might not be well informed by enough evidence to proceed quickly but must regardless. Whatever the nature of the emergency, it is the very nature of catastrophes that they catch people unprepared; in recent history we’ve seen bushfires, floods, earthquakes, tsunami, storms, volcanoes, landslides and winds. The events are diverse in nature, but the effect on people is consistent and devastating.
It is the nature of emergencies that they are sudden and catastrophic (Galambos 2005). A swift turn of events means that some people lose their lives and other lives are put on tenterhooks. The initial damage tends to be physical and material, but mental health issues follow close behind. Whatever the emergency event; be it tsunami, bushfire, storm, flood or earthquake, the initial impact of the disaster only spells the beginning of the catastrophe. Because of supply interruptions, provisions for basic needs such as communication, shelter, food, sanitation and water as well as health services and social networks, matters tend to deteriorate after the initial shock. It is at this early stage when mental health issues begin to compound a disaster.
It is a conceit to think of mental and physical health as separate issues. Although they are distinct, the two are intimately related. One will exacerbate the other1. That is, mental stress tends to make physical illness worse and vice versa. For this reason it is imperative that service providers address mental issues as quickly and appropriately as possible after a catastrophic event, just as they will food, shelter and sanitation.
Delays in the provision of all forms of emergency care can be caused by indecision about what is suitable action. The question of appropriateness always calls for normative decisions based on subjective opinion – and those opinions are difficult to justify in life and death situations – especially when providing a limited resource to one person might mean someone else will go without. The outcome, sadly, is that decisions sometimes aren’t made and this only makes matters worse. It is for the psychological comfort of the decision makers that they (we) want to rely on evidence to make decisions. Evidence based decisions are easily justified and move the burden of decision making to scientists elsewhere. And fair enough. There’s little doubt that empiricism is the most suitable way forward in the circumstances where empirical evidence exists and is available at hand (Galambos 2005). This is, sadly, rarely the case.
The scientific method is very specific and conclusions can only be proven if they are drawn in isolation from any confounding variables that might otherwise influence the data. Not just is this clinical approach divorced from reality, but more significantly, the findings tend to be incremental and as such there isn’t enough empirical data to answer most basic real world problems. I am an architect and I specialise in mental health design2. Like emergency services provision, there is a huge onus on evidence to generate any innovations in this area of the profession. As with emergency services provision, evidence is time consuming to locate and analyse, and in many cases it turns out to be irrelevant in any case. There are few clients who are willing to encumber their design bills with much time for research, and yet, decisions need to be made constantly because architectural problems are incredibly consequent. One minor change here will affect something else elsewhere. Like the problems that face providers for emergencies, the problems we face are incredibly complicated and open ended, often with no clear solutions. Thus we usually have two ways forward. To continue to do things the way they have always been done – even if we suspect those methods are dated or plain wrong. Or we have to take risks and improvise. But I have been faced with these problems and have tried both methods and found them both deficient – so I developed a methodology that allows reasonable decisions to be made on the fly. And the same methodology can be easily adapted to enable quick and appropriate decision making for various logistical tasks in emergency situations.
Firstly it is important to understand that every provision means the denial of something else because resources are always limited in some way. It’s like going and ordering at a restaurant. Out of the twenty dishes presented you’ll only get to choose one. If the choice is yours, there’s a fair chance it will be the best choice. If the choice is left to someone else – your spouse for example, you might be disappointed. The defence that ‘beggars can’t be choosers,’ is unhelpful. It is not the spirit of fine dining to be classed as a beggar! Significantly, the more victims of emergencies can be spared a similar attitude the better.
Aaron Antonovsky’s salutogenic theory (1987) demonstrated that the distinction between sickness and health is indistinct and a person’s level of well-being will be somewhere on the continuum between death and a theoretical state of perfect health. Antonovsky found that a person’s state of health reflects a person’s sense of coherence. The more a person feels they understand and make a contribution to the world around them, the stronger their resistance to illness.
Figure 1: Antonovsky's salutogenic theory (1987)
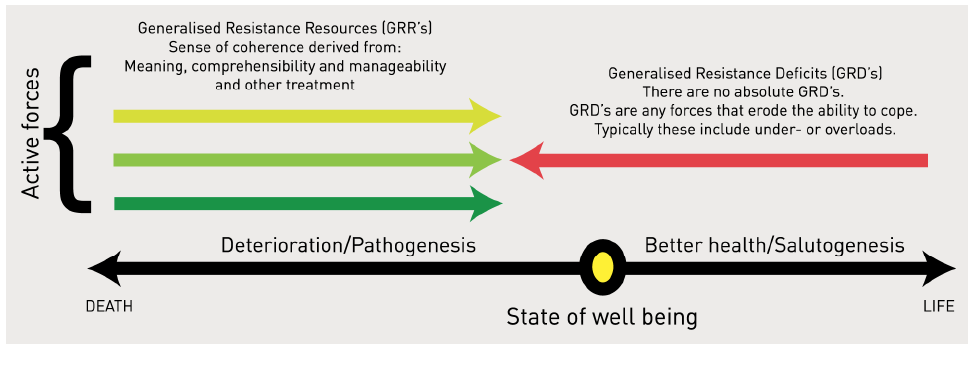
Antonovsky breaks down a sense of coherence into three domains of importance. A strong sense of coherence is supported by feelings of comprehensibility, manageability and meaningfulness (Golembiewski 2010, 2012). Ultimately a SOC builds a dynamic feeling of confidence that one’s internal and external environments are predictable and that there is a high probability that things will work out as well as can reasonably be expected (Bahrs, Heim et al. 2003). These categories can be extrapolated to find easy application in emergency situations as a salutogenic method. When applied to emergency care, comprehensibility is the matter-of-fact understanding of the situation a subject finds him or herself in. In a disaster situation this can mean information; who, why, what, where, how and when. Manageability, the next of the principles of salutogenic theory extrapolates to mean action and empowerment and in an emergency situation it will be the things that enable survival, things like food, water, communication, shelter and things that can be done to lessen the impact of the disaster. Meaning is the most illusive of all the salutogenic principles, yet it is in many ways the most important. Meaning always comes into question during disasters, yet it is the hardest issue to address. Meaning is the subject of the big question; “but why?” If meaning can be sustained, then survival in the most difficult and horrific circumstances becomes possible (Frankl 1963). This kind of survival gives others hope. It is the stuff of miracles, and it is through these miracles that meaning is fostered in others.
A salutogenic methodology for emergency care ensures that the best interests of the victims of disasters are always maintained with a holistic perspective, even when dealing with the minutiae of service provision. It is an approach to understanding the individual’s needs holistically and in such a way that the effort isn’t likely to interfere with the psycho-social needs of the subjects. This method is intended to be used by communication officers through to people at the cold face because it is simple to remember and easy to apply. It’s just a matter of keeping three things at the forefront of mind: Comprehensibility, manageability and meaningfulness, and having an idea of how these concepts work on the ground. With more complex projects (such as architecture or emergency service provision), each decision can be analysed with respect to the three salutogenic categories to see how elements relating to a sense of coherence can be incrementally supported. It is important to remember that this method is designed for use on the fly and mistakes are okay, to make an error of judgement using a salutogenic theory is better than having no theoretical basis whatsoever.
Comprehensibility is maintained when people are kept abreast of what’s happening. In the case of the Victorian fires, there was a need for information about where the fires were heading and at what velocity. Information is also needed about the emergency response. When will help arrive? People need to know who is dead and who survived. They need to know about the safety of their family, friends, pets and livestock. They need to know if their homes are in danger or if there is anything left of them. These are all very profound issues and quality information is an extremely important tool for the maintenance of a sense of coherence. The inverse is also true. Rumours and lies are harmful (Freyd, Klest et al. 2005). And so too can be ‘shielding’ survivors from the truth (although this is a complex issue in itself because the truth is rarely definitive and hope must also be maintained as much as possible). It might be really tough to tell a mother that her child has died, but if it is absolutely and unavoidably true, there is no protecting her from that fact. Yes, sympathy is called for and it might be ‘the last straw', but it is an inevitable last straw, and at the very least it shouldn’t come with added ugliness from deceit and distrust (Meyer 1969).
When information is given in an emergency, accuracy and honesty is imperative. Under promising allows expectations to be exceeded, carrying a strong message of hope and that everything is working out as well as possible. Disappointment on the other hand might be taken as betrayal. The art of making promises has implications for higher levels of coherence. When stressed, people might be excused for making unreasonable demands. They might, for instance, extract promises that are difficult or impossible to keep. Who, after all, wants to deny someone who is desperate and might have his or her life in danger? Who wouldn’t prefer to lie and say, ‘don’t worry. Everything will be fine?’ But a hastily made guess that ‘someone will be there to help in a couple of hours,’ can start doing damage at 120 minutes and 1 second (Alomes 2009). The reason is because the promise suddenly becomes questionable, and at this point meaning starts to erode (Golembiewski 2009).
Whether it is the provision of food, water, shelter, blankets or medical services, most aid and emergency provisioning focuses on improving manageability – usually helping people to help themselves. Its critical, but the obviousness of this area of concern tends to dominate emergency provisioning. Needs – physical ones are the squeaky wheel of emergency care. Information and material support enables people to act. And when people act, and feel that they can do something, their overall sense of coherence improves. This is good for health outcomes, and having people move from stunned/disabled mode to being an active participant in the rescue effort means another hand (with local knowledge) at the helm.
The absence of the things that make life manageable has obvious consequences, although they are not as significant as we tend to assume. Lack of food, water and shelter will be a source of stress that will make outcomes worse, but with meaning and comprehensibility needs looked after, people can go a long time without basics. As Frank Lloyd Wright famously said, “give me the luxuries of life, and I’ll gladly go without the necessities.”

San Francisco earthquake.
Meaning is the most difficult aspect of the salutogenic theory to understand and to provide for, but it is nevertheless the most important. Meaning is the glue of life. It is what makes lives whole and fulfilled. In psychotherapy, it is only when our life’s narratives are revealed to be meaningful that there is release and resolution (Clarkson 2006). Meaning is the force that binds social groups together and is a major purpose of religious belief (Obeyesekere 1981, Dirkheim 1976) All aesthetics, literature, art, and all other ubiquitous abstracts of human endeavour relate to and contribute to meaning (Golembiewski 2012). Meaning gives people the power to withstand inhuman conditions, starvation, illness, and extreme conditions (Frankl 1963). There are theories about why and how meaning gives people such tenacity, but it is not the purpose of this paper to go into these debates (For more information, see Golembiewski 2009).
Whilst meaning is associated with arts and the complexities of culture, there is no suggestion that reading poems will be of any use to someone who has just lost their family in a bushfire (on the other hand, it might happen to be just what’s needed!) In emergency situations meaning can be defined as whatever is of critical importance to the subjects. It means concern for life, for the people they care about, and sometimes for significant cultural constructions like religion, history and tradition. Meaning is what creates the desire to stay alive. And the desire to stay alive keeps people alive. Meaning comes from anywhere and everywhere, but there are some sources that are especially potent. Sometimes the emergency effort itself can contribute meaning, after all, being needed is a big one. Emergencies are situations where the people who are needed, are needed to the extreme. Thus involvement in the rescue operation is a good way to help people through their grief and hardship. This is true to the extent that fire-fighter’s have commonly been found to be arsonists, lighting fires, so they can fight them and feel significant as humans. By fighting fires, the arsonists found camaraderie and intense personal narratives, both of which are critically important contributors to a sense of meaning (Australian Institute of Criminology 2005).
Under normal circumstances meaning is a stable constant for most people. It waxes and wanes a bit, but in circumstances of extreme displacement it becomes mobile. Meaning is based on a personal ontology – a holistic foundation of connections, meaningful associations and distinctions and narratives that are created throughout a person’s entire life. As things are found to ‘make sense’ they contribute to this holistic body of knowledge and order. And things that don’t make any sense and cannot be understood directly challenge a person’s ontology, causing severe disturbances until everything makes sense again (Golembiewski 2009). In emergency circumstances meaning can be a double-edged sword. The power of meaning to do good by maintaining a person’s psyche can suddenly come under fire. The elusiveness of meaning means that it is particularly susceptible to inversion. Meaning can suddenly become meaninglessness – especially in extreme circumstances. And meaninglessness undermines a salutogenic framework like nothing else can. This causes bizarre and frightening expressions such as mutism or emotional shut-down (Reach Out 2009). In fact, there is every possibility that the atomisation of an ontological framework is the root cause of every single case of mental illness – especially the psychoses (Searles 1966; Golembiewski 2009).
The capacity for the ontology to flip makes the protection of meaning the single most important function of the emergency caregiver. The well-accepted model proposed by Maslow (the hierarchy of needs model), places meaning as a ‘higher’ need that can only be considered once the stability of ‘lower’ needs such as shelter or food is established. This truism is false. Rather it is the ontology the ‘highest need,’ that is the foundation upon which everything is known. The ontology is the product of self-actualisation. Without a strong ontology, a person loses the capacity to think, feel, or even act. But people can go without basic needs or make do indefinitely if the struggle is meaningful. There is meaning in place and even in the narrative of hanging in there against the odds.
Of course the maintenance of someone else’s body of wisdom and experience isn’t possible because we still have no means to occupy somebody else’s mind. So how can we help? We can be on the lookout. As we know that emergencies trigger ontological challenges we can encourage people to find direction when they most need it. Getting survivors active and involved in the emergency effort when they look like they might otherwise take a turn for the worse can be a good idea. We can be encouraging, helping the survivors of disaster understand that all that is humanly possible will be done and that the things will work out as well as can reasonably be expected. It is important, however not to overplay this, as dashed promises or misinformation are often the tipping point to despair (Alomes 2009). In catastrophes, the survivors must be allowed to feel that they can trust the providers and care they are getting. Consider the anger after Hurricane Katrina when misinformation about looting caused the mobilisation of armed troops with orders to shoot. The McLeod Commission noted that the greatest failure of the bushfire response was the misinformation that the response team disseminated in good faith (McLeod 2003).
Frequently ontological shifts mean that old spiritual models will be dismissed. In these circumstances missionaries for various faiths can do a lot of good, even as they prey on the victims of disaster. Rigid belief systems offer support when it is most needed, like a crutch, but have a tendency to fail people down the track (Antonovsky 1987). In emergencies missionary activity can be a double edged sword of its own – often missionaries are very experienced and generous caregivers who ask nothing in return, but cultural suitability of service provision is an issue that cannot be overlooked. Culture is a very important source of meaning and is a context for our life’s narratives.
When Nero famously played the fiddle while his city burned, was he mad or was he reaching for the thing that gave him meaning and a sense of control at a time of extreme disempowerment and inevitable death? In emergency situations even empirically tested and well-accepted theory and information may not apply. Catastrophes both change the normal order of things and the speed with which decisions have to be made. So it is essential that people who are to go out and face emergencies are equipped to make clever decisions on the fly. An extrapolation of salutogenics (a salutogenic method), is a fine tool for such circumstances, because it is easy to guess how little efforts might be amplified once projected onto a simple salutogenic framework; how does an action affect manageability, comprehensibility and the sense of meaning? Is the sum force on the coherence continuum likely to be life supporting or not?
References
Alomes, V. (2009). Alive and Well; A new and total approach to suicide prevention and community well being in rural areas. Australian Rural and Remote Mental Health Symposium. Canberra, Beyond Blue National Depression Initiative.
Antonovsky, A. (1987). Unravelling the Mystery of Health. San Francisco, Jossey-Bass Inc.
Australian Institute of Criminology (2005). Firefighter arson. Canberra, Commonwealth of Australia.
Bahrs, O., S. Heim, et al. (2003). Salutogenesis in General Practice; How to use the Potential of Doctor-Patient-Communication to Promote Health 2nd Conference on Making Sense of: Health, Illness and Disease. St Hilda’s College, Oxford.
Bunk, S. (2004). World on Fire. Public Library of Science. Northwest_Crown_Fire_Experiment.png. Northwest Territories, Canada.
Carson, N. (2009). Smoke mixes with clouds over Warrandyte on the afternoon of the 8th of February. Looking northeast. 2009_bushfires_Warrandyte_wikicommons.jpg. Warrandyte, Wikicommons.
Clarkson, J. D. (2006). The Dream Not Yet: a journey into the not so mystic wold of psychotherapy. Claremont, Western Australia, J G Clarkson Assoc.
Ellsworth, W. L. (1990). The San Andreas Fault System. Earthquake history, 1769-1989. R. E. Wallace (ed.). California, United States Geological Survey. 1515: 152-187.
Factoryjoe (2009). Maslow’s hierarchy of needs under creative commons licence, Wikicommons.
Frankl, V. E. (1963). Man’s Search for Meaning: An Introduction to Logotherapy. New York, Pocket Books.
Freyd, J., B. Klest, et al. (2005). “Betrayal trauma: Relationship to physical health, psychological distress, and a written disclosure intervention.” Journal of Trauma & Dissociation 6(3): 83-104.
Galambos, C. M. (2005). “Natural Disasters: Health and Mental Health Considerations.” Health and Social Work 30(2): 83-87.
Golembiewski, J. (2009). We are our architecture. Science and Non-duality Conference. San Rafael, California, Centre for Consciousness Studies, (University of Arizona) Available through; Conference recording.com. SND29-315 DVD 3/3.
Golembiewski, J. (2010). “Start making sense; Applying a salutogenic model to architectural design for psychiatric care.” Facilities (Emerald Publishing Group PLC.) 28(3).
Golembiewski, Jan. (2012). So you’re going to design a mental health facility? How to make it future-proof. World Health Design Scientific Review, 5(2), 74-79.
Golembiewski, J., B. Ho, et al. (2004). Shelter. In P. Droege & S. Hawken (Eds.), Bangun: A response manual for tsunamis and other natural disasters (pp. 3.1-3.24). Sydney: UNSW. ( http://www.fbe.unsw.edu.au/courses/bangun/manual.asp ) This is an open source resource. No rights have been retained.
Johnson, K. (2009). Awakening in prison. Science and Non Duality Conference. San Rafael, Centre for Consciousness Studies, (University of Arizona). SND C14
Little, A. (2009). Service network approaches to supporting rural communities following disasters. Australian Rural and Remote Mental Health Symposium. Canberra, Australia New Zealand Mental Health Association.
McLeod, R. (2003). Inquiry into the Operational Response to the January 2003 Bushfires in the ACT. ACT, Department of the Chief Minister.
Meyer, B. (1969). “Truth and the physician.” Bulletin of the New York Academy of Medicine 45(1): 59.
Obeyesekere, G. (1981). Medusa’s Hair; an essay on personal symbols and religious experience. Chicago, University of Chicago Press.
Quo Vadis (1924). Quo Vadis poster. Rights expired.
Reach Out. (2009). “After someone has died.” From http://au.reachout.com/find/articles/after-someone-has-died.
Records of the Office of the Chief Signal Officer (1906). San Francisco Earthquake, National archives and Records Administration.
Searles, H. (1966). “Concerning the development of an identity.” Psychoanalytic Review 53(4): 7-30.
About the author
Jan Golembiewski is an architect and neuroscientist. He is a specialist in architecture to improve patients' sense of well-being.
Footnotes
1. This is true in situations where the emergency was an unusual occurrence. In situations where emergencies are regular and expected, such as in the North East of NSW, which is subject to frequent flooding, events cause some psychological stress, but probably don’t trigger mental illness as such (Little 2009).
2. I also have some experience with emergency services provision; I was part of Bangun, a UNSW effort to assist survivors of the 2004 Boxing Day Tsunami. (Golembiewski, Ho & Wong 2004)